

























































































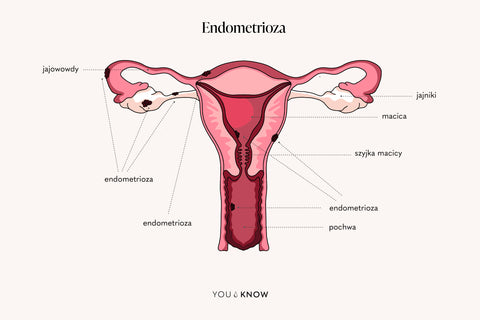
Inspired by questions in the endometriosis group and Google searches, we have prepared another post about endometriosis.
Does endometriosis cause infertility?
Endometriosis is undoubtedly a possible cause of infertility. At the level of the immune system, inflammation and the body's immune response do not favor the creation of an environment favorable to fertilization. An additional problem is embryo implantation. Scientific studies have confirmed that the endometrium of people with endometriosis differs in terms of receptors and immunologically from the endometrium of healthy people. Studies that determine which came first: the "egg" or the "chicken" are still ongoing. They try to answer the question of whether the endometrial cells are "different" and cause the development of endometriosis, or whether the disease comes first and the cells change under its influence.
Peritoneal adhesions in endometriosis
Adhesions in the pelvis disrupt the proper functioning of the pelvic organs – I mean blocked fallopian tubes or distortions of the ovary-fallopian tube relationship. As a result, the egg cell is not fertilized or the fertilized cell cannot reach the uterine cavity, which additionally promotes the development of ectopic pregnancies, the subject of which we will expand on later.
Infertility and sterility – what is the difference?
First, let’s clear up some theory. The WHO defines infertility as “the inability to achieve pregnancy after a 12-month period of regular sexual intercourse (2 to 4 times per week) without the use of contraceptive methods.”
Infertility is divided into female and male, as well as primary and secondary. While we have no doubts about the first division, because it is simply about the type of sex cells produced, in the second we are interested in the fact whether there was ever a pregnancy before the infertility was diagnosed. If so, we are talking about secondary infertility, if not, primary. And it is exactly as you suggest in your questions: we are still struggling with infertility, while infertility is a final state (related to, for example, the removal of a reproductive organ).
Ovarian reserve and AMH testing in endometriosis
Another problem is the reduction of ovarian reserve due to endometrial cysts. They can destroy the structure of the ovary, contributing to a decrease in reproductive potential. And how do we actually determine ovarian reserve? During the visit, the first thing we do is an ultrasound. We determine the number of antral follicles, i.e. the smaller ones that may become the dominant follicle in the future and play the main role duringovulation . If there are fewer than 4, a red flag goes off and we start to delve deeper into the subject.
In addition to assessing FSH, LH and estradiol (the most frequently tested hormones), we also assess AMH, or anti-Mullerian hormone. The fewer follicles, the lower its level. But don't worry - if you don't have other adverse factors (previous ovarian surgery, chemotherapy, radiotherapy, smoking or older age), your body will cope with this problem.
I would also like to point out that a low ovarian reserve diagnosis is not a sentence and does not mean that you will not get pregnant naturally. There is an option that you will have to try for a little longer, possibly monitor your cycle and take medication, and in the case of infertility diagnosis, seek advice from a doctor who deals with such problems. We live in the 21st century and we have a whole range of assisted reproduction methods. It is important not to postpone this visit until the last moment with low results and to consult a specialist.
Surgical treatment for infertility – friend or foe?
Surgery is still a controversial topic among specialists treating patients with endometriosis. Does diagnostic laparoscopy make sense in endometriosis? Is it worth operating on small, asymptomatic cysts? On the one hand, they remove macroscopic foci that increase inflammation in the body and in many cases help patients get pregnant; on the other hand, we must remember that every intervention carries the risk of adhesions, which are not our allies either. Each situation should be considered separately, so I emphasize once again: trust your doctor.
Assisted reproductive methods
Girls, don't waste your time wandering from gynecologist to gynecologist. Infertility treatment should take place in a place designated for this purpose - in an infertility clinic. And what options await you there? There are special guidelines for treating patients with infertility and the doctor makes a decision based on several factors: age, medical history and test results. It is possible to perform intrauterine insemination (although its validity is disputed in people with advanced endometriosis), additional hormonal treatment and in the most difficult cases - IVF ( in vitro fertilisation ). And let's agree that when it comes to the "beginning of the stairs" of trying to get pregnant, i.e. ovulation monitoring and possibly supportive drug therapy - then we act! But when a patient who has been struggling with infertility for several years comes to my office, I perform an ultrasound, cytology, and then have an honest conversation with her, order a package of specialist tests and recommend a specialist dealing with infertility treatment. For these women, time is of the essence, which is why I want them to see a doctor as soon as possible, who will know what direction to take based on initial tests.
Endometriosis and IVF pregnancy
According to the guidelines of the Polish Society of Reproductive Medicine and Embryology, in vitro fertilization, or IVF, is a method intended for patients with moderate and advanced endometriosis, stage III and IV. When do patients with stage I and II endometriosis have indications for IVF? This is the next stage of the procedure, after conservative treatment proves ineffective. Each patient with endometriosis must be approached very individually (as in the treatment of endometriosis itself). And it is not only about the advancement of the disease, but also age, BMI and the entire medical history, which is why an individual approach is so important.
Endometriosis surgery before IVF?
What if we have macroscopic endometrial changes? We need to prepare for the entire procedure appropriately. According to the recommendations of the aforementioned Society, in the case of a hydrosalpinx, the fallopian tube should be cut out or its uterine end should be considered. Otherwise, the presence of the change can reduce the effectiveness of the IVF procedure by 50%. When it comes to endometrial cysts, surgery is not recommended for changes that are less than 4 centimeters. The surgical procedure has a greater negative impact on the probability of pregnancy than the presence of the cyst itself.
Does endometriosis surgery increase the likelihood of getting pregnant?
Here we come to a question you often ask: does laparoscopy increase the chances of getting pregnant? It depends on many factors. Another procedure concerns the situation described above, i.e. when you are determined to get pregnant, do not want to or cannot wait any longer.
We act completely differently when you are of reproductive age and you think about your chances of getting pregnant in a few years. In such cases, pharmacological treatment is a better solution (of course, everything under the supervision of a specialist), because the more surgeries, the more adhesions and interference with ovarian tissue. I would like to point out here that the situation is completely different with changes that, despite pharmacotherapy, remain symptomatic. Then surgery and removal of the changes are necessary - if possible all of them. As you can see, the matter is really complex and the treatment of endometriosis is highly specialized. Find out from our other article what endometriosis surgery looks like .
Adenomyosis and pregnancy
The next issue you asked about was adenomyosis, or endometriosis of the uterine muscle, the main symptom of which is painful periods. Here, it's not so easy, because we can't just cut out the "problem," because that would involve removing the uterus. And does adenomyosis affect fertility? Basically, yes, considering its immunological effects. In addition, adenomyosis is closer to the endometrium (the vicinity of the uterine muscle and its mucosa), where the embryo nests. But there is also another version of adenomyosis: it often occurs in women who have already given birth. However, the mechanisms of its development are still not entirely clear to us.
Does endometriosis increase the likelihood of miscarriage?
Despite all the odds, you got pregnant, but unfortunately it ended in a miscarriage. Does endometriosis increase the likelihood of miscarriage? Most studies have shown that in the first trimester, yes. This is related to improper embryo implantation and the functioning of the immune system. The authors emphasize the importance of educating patients on this issue, but at the same time reassure them. Don't worry, the fact that you are being treated for endometriosis does not have to cause a miscarriage.
Endometriosis and ectopic pregnancy

In patients with endometriosis, the probability of ectopic pregnancy increases, i.e. one in which the fertilized cell did not implant in the uterine cavity (so-called ectopic pregnancy, about which you can read more here ). Its most common variant is a tubal pregnancy - fertilization occurred, but the fallopian tubes did not fulfill their function and did not transport the embryo to the uterine cavity. As I mentioned earlier, adhesions predispose to this, which arise not only due to endometriosis, but also procedures in the reproductive organ, as well as as a result of pelvic inflammatory disease. Meta-analyses indicate a possible relationship between the occurrence of ectopic pregnancy and endometriosis, while emphasizing that we need more well-designed studies. The complicated immunology of this disease and the inflammation of the reproductive organ that is produced are also important.
The impact of endometriosis on pregnancy
The good news is that in most cases this nasty disease will not stand in the way of women planning a pregnancy and after a shorter or longer struggle you will achieve your goal. According to most studies and observations, endometriosis is "quieted" during pregnancy, which makes you forget what the symptoms of endometriosis are. This is due to hormonal changes, and consequently immunological changes that occur during pregnancy. However, there are exceptions to this rule. While an endometrial cyst that forms in advanced pregnancy will not affect its course, there are other risks (for example, the aforementioned miscarriages in the first trimester).
What is more, the previously mentioned hormonal changes contribute to changes in the ultrasound appearance of cysts – sometimes they resemble neoplastic changes. In such cases, additional Ca 125 tests are of no use to us – during pregnancy, this indicator is usually elevated and will not help us differentiate endometriosis from cancer – and the mere suspicion of cancer is an indication for surgical treatment.
The surgeries are most often performed in the second trimester of pregnancy, considered the safest period for this type of intervention, taking into account both the development of the fetus and possible uterine contractions. Each case must be considered individually not only by a team of gynecologists, but also by obstetricians. It is important that the surgery is performed in a center experienced in such cases. The patient will be properly qualified for the surgery, will receive drugs that reduce uterine contractility, and the procedure will be performed by an experienced gynecologist. But here I also appeal for calm - not every cyst during pregnancy needs to be operated on. These are incredibly rare situations and require a consensus on the benefits and risks for both the mother and the fetus.
Endometriosis in the cesarean section scar
You gave birth to a child, you are a mother. But unfortunately this may not be the end of adventures. As I mentioned in the post about endometriosis diagnosis , it can nastily implant itself in the perineal wound after a natural birth or a postoperative wound after a cesarean section.
Terrible pain during menstruation, a palpable lump in the scar projection – these are standard symptoms of endometriosis. During my last shift, I saw another symptom – I must admit, for the first time in my life – a huge “haematoma” that appears during every menstruation, located all over my abdomen. I have never seen anything like this, and for this woman, it is a story that repeats itself every month. She has an additional “menstruation” in the subcutaneous tissue, hence the purple-red color.
How is endometriosis treated in a cesarean section scar? It simply involves cutting it out during what is supposed to be a very small procedure. We cut a small section of the scar, find the lump, cut it out and sew it up. But how many times has it turned out that this small lump in the subcutaneous tissue is the tip of the iceberg – and that endometriosis penetrates all the way to the muscle and its fascia! Sometimes the surgery ends with the use of a mesh, because we cut out such a large fragment of tissue that its continuity can be recreated.
Does surgery make sense if you are trying to have a baby? No, if you are giving birth by caesarean section (yes, that is also childbirth!) – then it can be removed during the procedure. And can it make it harder to get pregnant again naturally? Endometriosis in the subcutaneous tissue – no. The question is what is happening inside your abdominal cavity and whether there are any changes there that are suspicious of endometriosis foci.
We can't give up!
Endometriosis is a multi-faceted disease that requires an individual approach at every level: from diagnostics and recognition through treatment of its symptoms to the destruction of changes. Slowing down the progression of the disease or endometriosis diet therapy are also important aspects . For many women of reproductive age, having a child is a very important issue, which is why they bravely fight the disease through pharmacological treatment, often surgical, as well as the infertility treatment discussed today. Girls, patience, perseverance and a lot of strength! We are with you!
Created at: 06/08/2022
Updated at: 16/08/2022